
At a time when structured conversations around ageing were almost non-existent, this initiative marked one of the first organised efforts to engage directly with the community on the realities of growing older. It was, once again, a pioneering step shifting the focus from reactive care to proactive awareness and preparedness.
Recognising that many of the challenges of old age stemmed from lack of foresight, a series of community-based workshops were designed and conducted, with a special emphasis on senior citizens. These sessions opened up much-needed dialogue on the often-unspoken perils of ageing, while also presenting a pathway towards a smoother, more secure later life.
These sessions opened up much-needed dialogue on the often-unspoken perils of ageing, while also presenting a pathway towards a smoother, more secure later life.
Through these workshops, elders were guided to understand the importance of self-care, timely medical consultations, and maintaining functional independence. Equal emphasis was placed on financial preparedness, balanced nutrition, emotional well-being, and the creation of dependable support systems.
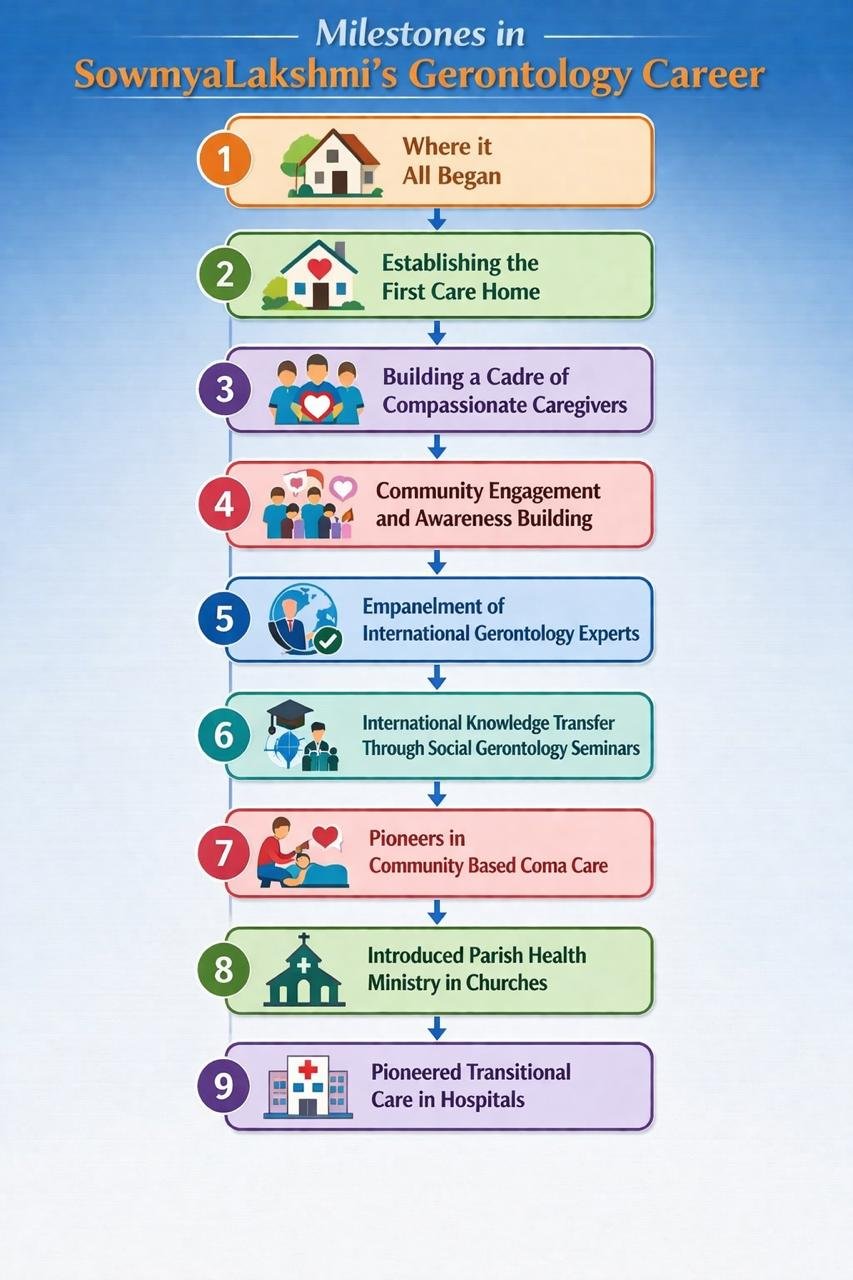
Parallel to these on-ground efforts, several thought-provoking articles on ageing and elder care were published in leading Kannada and English dailies. These writings carried the message into a much wider public domain, helping to sensitise families, caregivers, and society at large. They played a crucial role in normalising conversations around ageing and reinforcing the importance of planning for later life.
What set this milestone apart was its multi-pronged approach, combining direct community engagement with public thought leadership. More importantly, it empowered seniors to take ownership of their ageing journey, shifting the narrative from passive dependence to informed and purposeful living. Ageing, thus, began to be seen not as a decline to be feared, but as a phase to be consciously planned, navigated, and lived with dignity.
At a time when the very term social gerontology was virtually unknown in India, both among the general public and within academic circles, we took a decisive and forward-looking step. Having been among the first to introduce and actively practice this discipline in the country, we recognised the need to anchor our work in global knowledge systems and established best practices.
With this vision, we initiated the empanelment of an international team of distinguished gerontology experts. Our objective was not merely collaboration, but meaningful knowledge transfer from well-established systems across the world, ensuring that our approach remained both contextually relevant and globally informed.
In our formative years, we were privileged to be supported by an impressive group of academicians and practitioners in the field of gerontology. What stood out was not just their expertise, but their willingness to handhold and guide us driven by a shared commitment to a larger cause. They recognised our passion and our earnest effort to bring social gerontology into the mainstream in India, at a time when the discipline itself was still in its infancy here.
Our international associates included Paul Nash (CA, USA), Judy Parnes (NJ, USA), Amy Cotton (Maine, USA), Carolyn Gallogly (Long Island, NY, USA), Ibby Tanner (Baltimore, USA), Robyn Flipse (NJ, USA), and Vanessa Burholt (Ireland). Their guidance and encouragement played a significant role in shaping our early direction and strengthening our foundation.